
Friday, May 13, 2016
Thursday, January 14, 2016
New Year, New You: Revamping Your 2016 Diet Without Breaking the Bank

It's the most wonderful time of the year! The holidays have passed, and the big, home-cooked feasts and hearty leftovers are finally gone. For those who want to revamp their health and wellness, the start of 2016 presents a blank canvas to paint a new picture and a healthier lifestyle.
Here are four easy tips to revamp your diet without breaking the bank.
1. Eat regular meals.
Missing a meal almost always leads to overeating at the next meal. As a result, it is super important to eat regular meals to maintain energy throughout the day and choose more balanced and nutritious foods. Meal prepping is a great way to make sure that you always have something to eat. Plan out your meals each day or week, and make sure to pack enough healthy options to keep you satiated throughout the day.
2. Drink water 30 minutes before eating.
 |
"Always start meals with a glass of water"- Shane Allen
|
One study recruited a group of 84 overweight adults for a 12-week experiment. Everyone was given general wight loss advice, then assigned to one of two groups. One group was told to drink 16 ounces of water 30 minutes before their meals while the other group was told to simply imagine their stomachs were full before meals. Findings showed that the group that drank at least 16 ounces of water lost an average of three more pounds than the group that didn't increase their water intake. Results also showed that the more water that participants drank before meals, the better their weight loss.
3. Don't grocery shop while hungry.
If you've ever gone grocery shopping while hungry, you know the tangled web you wove. On an empty stomach, everything in the grocery store looks gooooooood, especially those Oreos and Zebra Cakes. As a result, it is best to avoid shopping while hungry. One study found that when compared to participants who had eaten before shopping, those who had not eaten were much more likely to purchase more high-calorie products.
4. Avoid diet sabotagers.
Diet sabotagers come in two forms: food and folks.
Certain foods are notorious for being high in fat, carbs, and sugars. These are the foods that you want to avoid if you are looking to adopt a healthier lifestyle or lose weight. Starchy carbs and sugary extras are diet sabotagers! Both pack on pounds much quicker and with negative side effects such as increased blood glucose levels.
People can also sabotage your diet (we all have that one friend who always wants to meet at the food trucks for lunch)! The key to success in these situations is having the willpower to say, "No," or finding a healthier alternative. For example, instead of meeting at the food trucks for lunch, suggest a walking lunch where the meeting not the food is the focus.
SOURCES
1. Stookey, JD, F. Constant, and BM Popkin. "Drinking Water Is Associated With Weight Loss in Overweight Dieting Women Independent of Diet and Activity." Drinking Water Is Associated with Weight Loss in Overweight Dieting Women Independent of Diet and Activity 16.11 (2008): 2481-488. Pub Med. Web. 14 Jan. 2016.
Wednesday, November 18, 2015
Gamechanger: Medicaid Expansion in Low-Income Populations
Background
Since it was signed into law in 2010, the Patient Protection and Affordable Care Act has been the subject of much political controversy. One polarizing
provision of the Affordable Care Act (ACA) is the expansion of Medicaid. Though Medicaid expansion was passed federally, the adoption of the expansion remains at the discretion of each state. Today, 31 states have adopted Medicaid expansion while 20 states have either not expanded or are still debating the issue.
Under current federal regulations, states must provide Medicaid coverage for children younger than 6 years of age with family income up to 133% of the federal poverty level, children ages 6 to 18 years with family income at or less than 100% of the federal poverty level, pregnant women, and low-income elderly persons (Kaiser Family Foundation). The ACA (1) expanded Medicare eligibility to uninsured, non-disabled adults without children whose family income is at or below 138% of the federal poverty level and (2) established state health insurance exchange programs that offer a variety of low-cost options for enrollment with variable benefit packages (Chesney, 313). These new provisions are projected to result in insurance coverage for 33 million uninsured people by 2022.
why expansion matters: Medicaid and access to care
why expansion matters: Medicaid and access to care

- Mary Chesney, PhD, RN, CPNP
Medicaid is the nation's largest provider of health insurance for children and adults. It insures over 65 million Americans, provides financial support for the nation's safety net institutions, and is central to increasing access to care for many of the most disadvantaged individuals and families in the United States.
Medicaid expansion significantly impacts access to care, health outcomes, and quality of care in vulnerable populations. Thirty-one million children (one in three) and more than 60% of residents in nursing homes depend on Medicaid to receive health care services (Center on Budget and Policy Priorities). Health insurance coverage is associated with better health outcomes because it grants individuals regular access to care and fosters greater and more appropriate use of health services. These factors, in turn, improve the likelihood of disease screening and early detection, the management of chronic illness, and effective treatment of acute conditions such as traumatic brain injury and heart attacks (Kaiser). Therefore, the ultimate result of Medicaid expansion is better health outcomes.
setting the landscape: medicaid expansion by state
Though the benefits of Medicaid expansion are well documented,
states have taken variable approaches to ACA Medicaid Expansion. A
recent study examined ACA-related experiences among low-income adults in three
states with markedly different ACA policies: Arkansas, Kentucky, and Texas (Sommers, 1010). The objective of the study was to assess the
experiences of low-income adults in each of the three states and explore
connections between state policy and enrollment in low-income populations.
The Medicaid expansion policies of Kentucky, Arkansas, and Texas
are compared in the table below.
State
|
Medicaid Expansion Adopted?
|
State Marketplace?
|
Outreach Efforts?
|
Kentucky
|
Yes, traditional Medicaid expansion
|
Yes
|
Yes, aggressive outreach by governor’s office, navigators,
and in-person assisters
|
Arkansas
|
Yes, private option
|
Yes, federal-state partnership Marketplace
|
Yes, in-person assistance only; ACA promotion strictly
prohibited
|
Texas
|
No
|
No
|
No, ACA promotion and use of navigators are strictly
restricted
|
Because of their disparate policies, Kentucky, Arkansas, and Texas have seen different results regarding ACA applications and enrollment among low-income adults. Study results indicate that low-income adults in Kentucky - and to a lesser extent in Arkansas- are much more likely to apply and enroll in Medicaid or other Marketplace plans than low-income adults in Texas (Sommers, 1011). These results reinforce the importance of accessible care in granting health insurance to those who need it the most.
The high accessibility and promotion of Medicare and the Marketplace has created a 52% decrease in the number of uninsured Kentuckians since 2013 (Duckett). According to a report published by the Kentucky Cabinet for Health and Family Services, 75% of Kentuckians who had signed up for coverage during the 2014 open enrollment session (391,000 Kentuckians) indicated that they had been uninsured prior to gaining insurance through the state exchange.
This unprecedented coverage is especially significant for those who previously did not qualify for Medicaid but could not afford private insurance. Through the expansion, individuals who fall in this coverage gap are granted access to Medicaid or low-cost private insurance plans that can save their lives in the long run.As a result, one can infer that the best way for states to improve access to care for low-income populations is to adopt Medicaid expansion. The expansion of these provisions will increase access to care, foster positive health outcomes, and help push disadvantaged populations toward health equity.
The high accessibility and promotion of Medicare and the Marketplace has created a 52% decrease in the number of uninsured Kentuckians since 2013 (Duckett). According to a report published by the Kentucky Cabinet for Health and Family Services, 75% of Kentuckians who had signed up for coverage during the 2014 open enrollment session (391,000 Kentuckians) indicated that they had been uninsured prior to gaining insurance through the state exchange.
final take-aways
Kentucky's success with ACA applications and enrollment is accredited to the state's adoption of the Medicaid expansion, the commission of a state marketplace, and aggressive outreach efforts that used a mix of the governor's office, in-person assistance, and navigators to assist applicants throughout the enrollment process. Similar measures in other states (Maryland, West Virginia, etc.) have also seen positive results. In contrast, states such as Texas who have restricted ACA expansion efforts have seen markedly less progress regarding declines in the uninsured population (17% in Texas compared to over 50% in Kentucky, Maryland, and West Virginia).This unprecedented coverage is especially significant for those who previously did not qualify for Medicaid but could not afford private insurance. Through the expansion, individuals who fall in this coverage gap are granted access to Medicaid or low-cost private insurance plans that can save their lives in the long run.As a result, one can infer that the best way for states to improve access to care for low-income populations is to adopt Medicaid expansion. The expansion of these provisions will increase access to care, foster positive health outcomes, and help push disadvantaged populations toward health equity.
sources
Chesney, Mary. "Affordable Care Act: Medicaid Expansion Key to Increasing Access to Care." Journal of Pediatric Health Care 27 (2013): 312-15. Web.
Duckett, Philethea, Artiga, Samantha. "Health Coverage for the Black Population Today and Under the Affordable Care Act." Kaiser Family Foundation (2013). Web.
Paradise, Julia. "Medicaid Moving Forward." Kaiser Family Foundation (2015). Web.
Sommers, B. D., B. Maylone, K. H. Nguyen, R. J. Blendon, and A. M. Epstein. "The Impact Of State Policies On ACA Applications And Enrollment Among Low-Income Adults In Arkansas, Kentucky, And Texas." Health Affairs 34.6 (2015): 1010-018. Web.
Paradise, Julia. "Medicaid Moving Forward." Kaiser Family Foundation (2015). Web.
Sommers, B. D., B. Maylone, K. H. Nguyen, R. J. Blendon, and A. M. Epstein. "The Impact Of State Policies On ACA Applications And Enrollment Among Low-Income Adults In Arkansas, Kentucky, And Texas." Health Affairs 34.6 (2015): 1010-018. Web.
Thursday, October 29, 2015
Closing the Gap: Increasing Truvada PrEP Awareness
Background
 On July 16, 2012, Truvada PrEP became the first FDA-approved drug for reducing the risk of sexually-acquired HIV in HIV-negative individuals who are at high risk for contracting HIV.
On July 16, 2012, Truvada PrEP became the first FDA-approved drug for reducing the risk of sexually-acquired HIV in HIV-negative individuals who are at high risk for contracting HIV.
Truvada is an oral pill that contains two medicines that are useful in preventing HIV: tenofovir and emtricitabine. Covered by both Medicaid and most private insurances, Truvada has been proven to reduce the risk of HIV infection by 99% when taken daily, 96% when taken 4 or more times per week, and 76% when taken twice per week (US Centers for Disease Control).
In San Francisco and Miami, two cities with large LGBT populations, pilot studies proved that Truvada usage significantly reduced the incidence of new HIV cases. A Kaiser PrEP study followed 657 mostly gay and bisexual men who were referred for evaluation and decided to start PrEP. To date, there have been no new HIV diagnoses among the 657 participants during the 2 and 1/2 years of follow up (Kaiser Permanente).
PrEP's success has significant implications for communities of color, which experience disproportionately high rates of HIV infection and mortality due to AIDS. Heterosexual black women and black gay and bisexual men are two groups most at risk for contracting HIV in the United States. Of the 1.1 million Americans infected with HIV, almost 50% (510,000) are Black (Centers for Disease Control).
The stark statistics concerning HIV and communities of color reflect large systematic and structural barriers and health disparities that underserved, minority communities face every day. Historical and contemporary inequalities in housing, education, employment, health care, and the rate of mass incarceration only reinforce these disparities.
Truvada Usage Gap
Closing the Gap: A Call to Action
Much of the burden of closing the gap and reaching the LGBT community rests on health care providers; however, an equally yoked portion of these endeavors necessitates grassroots efforts in which individuals work within communities to spread awareness and reach people where they are.

Two Simple Ways to Advocate
1. Get informed: Know your status, read unbiased literature, find out where to refer friends and family members for more information, ask your health care provider about Truvada PrEP.
2. Share information: Adopt the "Each One Teach One" mindset by telling family and friends about the information that you've learned (particularly those that are high-risk for HIV), join advocacy or information groups such as PrEP-O-Licous, and share relevant updates and information on social media.
SOURCES
Kaiser Permanente San Francisco. Division of Research - HIV Care and Prevention. Large Study of PrEP Use in Clinical Practice Shows No New HIV Infections. Kaiser Permanente Share. N.p., 1 Sept. 2015. Web. 29 Oct. 2015. <http://share.kaiserpermanente.org/article/large-study-of-prep-use-in-clinical-practice-shows-no-new-hiv-infections/>.
Robinson, Russell, and Aisha Moodie-Mills. "HIV/AIDS Inequality: Structural Barriers to Prevention, Treatment, and Care in Communities of Color." Center for American Progress. University of California, Berkeley, 27 July 2012. Web. 29 Oct. 2015.
Volk, Jonathan, Julia Marcus, Tony Phengrasamy, Derek Blechinger, Dong Nguyen, Stephen Follansbee, and C. Bradley Hare. "Clinical Infectious Diseases." No New HIV Infections with Increasing Use of HIV Preexposure Prophylaxis in a Clinical Practice Setting 61.10 (2015): 1601-603. No New HIV Infections with Increasing Use of HIV Preexposure Prophylaxis in a Clinical Practice Setting. Oxford University Press. Web. 29 Oct. 2015.
United States. Centers for Disease Control. Department of Health and Human Services. PrEP Guidlines. N.p.: n.p., 2014. Centers for Disease Control. Web. 29 Oct. 2015. <http://www.cdc.gov/hiv/pdf/prepguidelines2014.pdf>.
HIV/AIDS disproportionately affects members of the LGBT community, and despite 30 years of research, there are still 50,000 new cases of HIV each year, two-thirds of which are among gay and bisexual men. - HRC Blog
On July 16, 2012, Truvada PrEP became the first FDA-approved drug for reducing the risk of sexually-acquired HIV in HIV-negative individuals who are at high risk for contracting HIV.Truvada is an oral pill that contains two medicines that are useful in preventing HIV: tenofovir and emtricitabine. Covered by both Medicaid and most private insurances, Truvada has been proven to reduce the risk of HIV infection by 99% when taken daily, 96% when taken 4 or more times per week, and 76% when taken twice per week (US Centers for Disease Control).
In San Francisco and Miami, two cities with large LGBT populations, pilot studies proved that Truvada usage significantly reduced the incidence of new HIV cases. A Kaiser PrEP study followed 657 mostly gay and bisexual men who were referred for evaluation and decided to start PrEP. To date, there have been no new HIV diagnoses among the 657 participants during the 2 and 1/2 years of follow up (Kaiser Permanente).
The Kaiser study is promising for HIV prevention because it extends what is known about PrEP from the controlled setting of clinical trials and shows that it can work in the "real-world". (Volk, 1202).Communities of Color
 |
| Black males account for 1-in-4 new HIV infections in the United States though they only make up 1-in-500 Americans, overall. - Reuters.com |
PrEP's success has significant implications for communities of color, which experience disproportionately high rates of HIV infection and mortality due to AIDS. Heterosexual black women and black gay and bisexual men are two groups most at risk for contracting HIV in the United States. Of the 1.1 million Americans infected with HIV, almost 50% (510,000) are Black (Centers for Disease Control).
The stark statistics concerning HIV and communities of color reflect large systematic and structural barriers and health disparities that underserved, minority communities face every day. Historical and contemporary inequalities in housing, education, employment, health care, and the rate of mass incarceration only reinforce these disparities.
Truvada Usage Gap
Thus, despite Truvada's life-changing benefits, lack of knowledge among health care providers, poor media coverage, and stigma have slowed the adoption of the drug, particularly in communities of color. In addition, many potential users have been driven away from health care and other services by negative experiences, overall distrust, and homophobia.
The persistence of abstinence-only education, failed incarceration policies, and resistance to harm-reduction programs combine to make the risk of acquiring, transmitting, and dying of HIV/AIDS higher in communities of color. Stigma is part of the problem as well. Many people within the Black community - particularly regular churchgoers - report that they would delay diagnosis and treatment due to embarrassment about sexually transmitted infections (Robinson).As a result, many of the people who could benefit from Truvada are not using it, either voluntarily or because they don't know that it exists. This creates a critical gap between Truvada's potential and actual usage and begs the question: What needs to be done to spread awareness, increase usage, and ultimately close the gap?
Closing the Gap: A Call to Action
Much of the burden of closing the gap and reaching the LGBT community rests on health care providers; however, an equally yoked portion of these endeavors necessitates grassroots efforts in which individuals work within communities to spread awareness and reach people where they are.
YES, YOU CAN BRIDGE THE GAP!
Two Simple Ways to Advocate
1. Get informed: Know your status, read unbiased literature, find out where to refer friends and family members for more information, ask your health care provider about Truvada PrEP.
2. Share information: Adopt the "Each One Teach One" mindset by telling family and friends about the information that you've learned (particularly those that are high-risk for HIV), join advocacy or information groups such as PrEP-O-Licous, and share relevant updates and information on social media.
SOURCES
Kaiser Permanente San Francisco. Division of Research - HIV Care and Prevention. Large Study of PrEP Use in Clinical Practice Shows No New HIV Infections. Kaiser Permanente Share. N.p., 1 Sept. 2015. Web. 29 Oct. 2015. <http://share.kaiserpermanente.org/article/large-study-of-prep-use-in-clinical-practice-shows-no-new-hiv-infections/>.
Robinson, Russell, and Aisha Moodie-Mills. "HIV/AIDS Inequality: Structural Barriers to Prevention, Treatment, and Care in Communities of Color." Center for American Progress. University of California, Berkeley, 27 July 2012. Web. 29 Oct. 2015.
Volk, Jonathan, Julia Marcus, Tony Phengrasamy, Derek Blechinger, Dong Nguyen, Stephen Follansbee, and C. Bradley Hare. "Clinical Infectious Diseases." No New HIV Infections with Increasing Use of HIV Preexposure Prophylaxis in a Clinical Practice Setting 61.10 (2015): 1601-603. No New HIV Infections with Increasing Use of HIV Preexposure Prophylaxis in a Clinical Practice Setting. Oxford University Press. Web. 29 Oct. 2015.
United States. Centers for Disease Control. Department of Health and Human Services. PrEP Guidlines. N.p.: n.p., 2014. Centers for Disease Control. Web. 29 Oct. 2015. <http://www.cdc.gov/hiv/pdf/prepguidelines2014.pdf>.
Tuesday, September 29, 2015
Depicting Obesity in Black America
DEPICTING OBESITY IN BLACK AMERICA
Overview
Obesity is a major health problem for millions of Americans. Dietary patterns, physical inactivity, medication use, and other exposures contribute to the prevalence of obesity in America. In an article, "Is Fat the New Normal?" Sherry Rauh likens obesity among Americans to tallness among basketball players. |
African American adults are 1.5 times as likely to be obese compared
with white adults, and over 75% of African Americans are overweight
compared with 67.2% of White Americans.
(State of Obesity - RWJ Foundation)
|
Rauh suggests that if we equate "normal" with average, it's not a stretch to say that in America, it's normal to be obese. The average or "normal" American adult's BMI is 28.6, which signifies overweight. The new normality of excess weight makes it very difficult for Americans to recognize what obesity looks like. This poses a serious concern in populations such as African Americans where obesity is highly prevalent.
Rush University MC Study
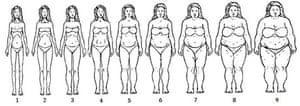
A study conducted by researchers from the Rush University Medical Center in Chicago, recruited sixty-nine African American women from a low income neighborhood of Chicago and asked them to identify which of the nine women (shown below) were overweight, obese, and "too fat". The consensus was that of the nine women shown, only 8 and 9 were "too fat" (Boosely).
Implications
This simple study conveys a larger disagreement between cultural and medical definitions of "healthy" in the African American community. This disconnect poses a much larger problem considering the effect of obesity on quality of life and risk for other chronic diseases such as diabetes, heart disease, hypertension, and some types of cancer. Since these illnesses are already disproportionately prevalent in minority populations, measures must be taken to mend this disconnect and push African Americans toward health equity.
What could be done?
1. Examination of social determinants of health that contribute to African American obesity. Determinants such as income, neighborhood, educational attainment, food advertising, and access to parks, grocery stores, and green space all play a critical role in the overall health of a community. African American communities face significant disparities in these determinants. Therefore, to help African Americans live healthier lives, these disparities must be eradicated. This will require strategic programs, policies, and neighborhood revitalization efforts that increase the availability and access to healthy food and safe space to be physically active in African American communities.
2. Development of culturally relevant healthy living and weight loss programs tailored to meet the unique needs of African Americans. To enhance cultural relevance and appeal to African Americans, these programs should solicit input from population members, use culturally relevant intervention content, incorporate population media figures, utilize culturally relevant forms of physical activity, and address specific population linked barriers to activity (Conn). For example, Steps to Soulful Living, a weight loss intervention for African American women, successfully reduced participants' weight by 8 - 15 pounds using these strategies (Karanja).
3. Use of nontraditional partners to increase health education in minority and low income communities. Instead of relying on traditional health education providers such as hospitals and clinics, providers should use nontraditional sources such as churches, community centers, sorority and fraternities, and barbershops/salons to conduct successful lifestyle interventions in settings that are both familiar and comfortable in the Black community (Kennedy et al).
Sources:
Boseley, Sarah. "Do You Know What Fat Looks Like?" Editorial. Obesity: The Shape We're In Blog. The Guardian, 10 Sept. 2014. Web. 29 Sept. 2015.
Conn, Vicki S., Keith Chan, JoAnne Banks, Todd M. Ruppar, and Jane Scharff. "Cultural Relevance of Physical Activity Intervention Research with Underrepresented Populations." Int Q Community Health Education34.4 (2013): 391-414. NCBI. U.S. National Library of Medicine. Web. 30 Sept. 2015.
Karanja, N., VJ Stevens, JF Hollis, and SK Kumanyika. "Steps to Soulful Living (steps): A Weight Loss Program for African-American Women." Ethnicity and Disease 12.3 (2002): 363-71. National Center for Biotechnology Information. U.S. National Library of Medicine. Web. 30 Sept. 2015.
Kennedy, Betty, Jamy Ard, Louis Harrison, Beverly Conish, Eugene Kennedy, Erma Levy, and Phillip Brantley. "Cultural Characteristics of African Americans: Implications for the Design of Trials That Target Behavior and Health Promotion Programs." Ethnicity and Disease 17 (2007): 548-54. Cite Seer X. Pennsylvania State University. Web. 30 Sept. 2015.
Rauh, Sherry. "Is Fat Normal in America? A Surprising Reason Why We're Gaining Weight." WebMD. WebMD, n.d. Web. 29 Sept. 2015.
The State of Obesity: Racial and Ethnic Disparities in Obesity. Rep. N.p.: Robert Wood Johnson Foundation, 2014. Web. 30 Sept. 2015.
Subscribe to:
Comments (Atom)